|
|
Giant Bone Island
General Considerations
- Bone islands (enostoses) are areas of mature compact bone in cancellous bone in the medullary cavity
- Usually oriented with its long axis parallel to the cortex
- Most common in pelvis, proximal femurs and ribs
- May change in size over time, but change usually takes years
Clinical Findings
Imaging Findings
- Round or ovoid
- Dense
- Greater than 2 cm in size (have been reported up to 10 cm in size)
- Spiculated, feathered or brush-like margin (also called “thorny radiation” “pseudophilia” “cumulus cloud appearance”)
- Thickening of trabecula
- No bone destruction
- No soft tissue mass
- Radionuclide bone scan usually shows no increased uptake
- MR: Loss of signal on all sequences, somewhat heterogeneous the larger they become
Differential Diagnosis
- Osteoblastic metastatic disease
- Osteosarcoma
Treatment
- None required
- If unsure of nature of lesion, follow-up in 3-6 months
Complications

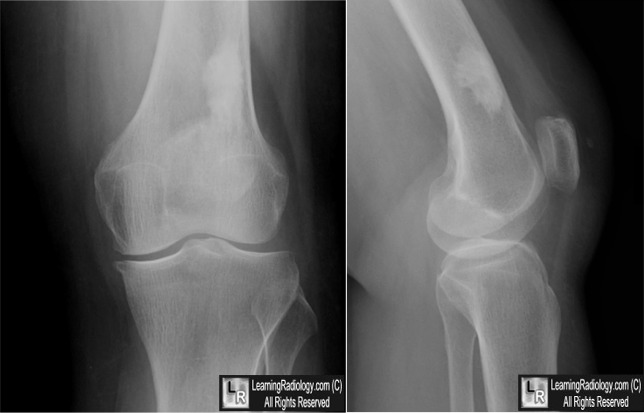
Giant Bone Island. Frontal and lateral knee radiographs show a large, well-circumscribed,
ovoid, sclerotic lesion in the distal femur (white arrow) with its long-axis oriented
parallel to the cortex and a spiculated (feathery) margin (yellow arrow).
For these same photos without the arrows, click here
For more information, click on the link if you see this icon 
Differential Diagnosis in Orthopaedic Oncology. A Greenspan, G Jundt and W Remagen. Lippincott Williams and Wilkins, 2006.
|
|
|

{kind=link}